Method for Marking the Upper Third of the Face Prior to Botulinum Toxin Therapy

Provision of high-quality medical care in the field of cosmetology requires not only the development of new medicinal products and methods of their application, but also solving organizational and legal issues, as well as professional training of a cosmetologist physician [3,12]. One of the important aspects in this area is the correct marking of the face before botulinum therapy.
The face is a distinctive individual characteristic of a person’s physical appearance and the most important informational zone [4]. A special role is attributed to the eyes and eyebrows, which psychologically form a holistic and specific image. The most expressive area of a person’s appearance is the region around the eyes. The eyes and the periorbital area are not without reason called the “mirror of the soul” [5].
The cornerstone of a creative approach to aesthetic correction and the effectiveness of botulinum therapy is knowledge of the anatomical and functional characteristics of the facial mimic muscles, understanding of the laws of facial expression, and mastery of botulinum therapy technique [14]. Correction of wrinkles and folds on the forehead, in the glabellar region, on the nasal dorsum, and in the periorbital area allows facial rejuvenation, which results in increased self-esteem and quality of life [13]. In the hands of a competent cosmetologist physician, the use of botulinum toxin type A (BoNT-A) injections can be compared to a brush in the hands of an artist [1]. The vast majority of adverse events are associated with the use of unjustifiably high doses of botulinum toxin and incorrect selection of injection points [6,7].
Documentation of indications and correction techniques is a form of protection for both the patient and the physician. Personal experience, aesthetic perception, and knowledge of the laws of proportion underlying beauty and attractiveness are required for a patient to say about a doctor: “He is a professional.” But how can anxiety at the beginning of professional practice, cosmetological disasters, mistakes, and complications be avoided?
Methods for correction of facial mimic wrinkles differ in technique, injection site, depth, dose, and staging. It is very difficult for a beginner cosmetologist physician to understand the correction methods described in published articles and monographs, especially since they often differ from the Instructions for medical use of the medicinal product.
Objective:
To develop a method for marking the upper third of the face prior to botulinum toxin therapy.
Materials and Methods:
Body image is the basis of a high level of self-esteem and self-confidence [10]. Dissatisfaction of patients with their appearance, especially after visiting cosmetologist physicians, may cause serious psychological disorders, which is also reflected in the general somatic status [2]. In recent years, the number of patient complaints to mass media, compulsory health insurance funds, consumer protection organizations, and judicial authorities regarding compensation for material damage and moral harm caused by the provision of inadequate medical care has been increasing [11].
Botulinum therapy is considered the “gold standard” for correction of age-related changes in the upper third of the face. When planning an injection correction scheme, the face should be considered as a single unit, and comprehensive correction is preferable.
Facial marking prior to aesthetic injection procedures is mandatory [8,9,15]. By drawing horizontal and vertical lines, a grid is created, into the quadrants of which injections are performed. External anatomical landmarks and muscle anatomy are used. Marking of BoNT-A injections according to the “traffic light” principle allows identification of:
- a zone of confident injection (green);
- an area of cautious injection in the presence of individual indications (yellow);
- an area where injections are not performed or require special justification (red) [9].
The objective of botulinum therapy in the upper third of the face is to reduce the visibility of wrinkles through relaxation of the forehead muscles, the glabellar region muscles, and the orbicularis oculi muscle while maintaining and/or forming the optimal eyebrow position and shape [9].
For injection botulinum therapy technique, the pupil and eyebrows are used as the basis for mapping, and the following method for marking the upper third of the face is applied:
I. Three main horizontal lines are drawn:
- 1 – at the level of the pupils when looking straight ahead;
- 2 – along the upper border of the eyebrows;
- 3 – in the forehead area, at least 2 cm above the supra-brow horizontal line (depending on the forehead height).
II. Main vertical lines:
- А – along the edge of the brow head (from the edge of the nasal ala to the beginning of the eyebrow);
- В – through the pupil;
- С – along the edge of the brow tail.
III. Additional reference lines (optional):
- а – fourth horizontal line – in the middle of the distance between the upper horizontal line and the hairline for second-row toxin injections (if necessary);
- b – from the pupil to the brow tail;
- c – from the pupil to the tragus of the ear;
- d – between the medial ends of the eyebrows and the contralateral inner canthus to determine the intersection point of the lines and injection into the procerus muscle;
- e – an additional vertical line along the lateral canthus margin.
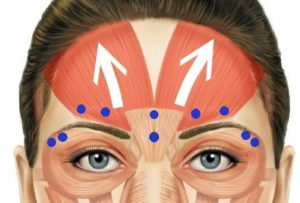
The intersections of these lines within the constructed grid determine the botulinum toxin injection points (see figure).

The prohibited zone for toxin injection is the area at least 2 cm above the horizontal line above the eyebrows. An exception for botulinum toxin type A injection into the frontalis muscle includes patients with individual anatomical features (low forehead).
Acceptable variations in injection point placement:
- In the lateral canthus area, lateral deviation of the basic point is acceptable (point 1C in the figure). The inferolateral point (Cc) may be shifted along line c toward the orbit (but not closer than 1 cm to the orbital rim), depending on the wrinkle pattern, when performing three injections along an arc with an interval of 1-1.5 cm from each other. Injection points in the periorbital area should take into account the eye type, shape, and width of the palpebral fissure [17].
- The location of injection points for BoNT-A in the forehead area may vary depending on the patient’s facial expression pattern. In the forehead area, a two-row injection technique is preferable. Injection points and their number in the forehead area should take into account the anatomical features of the frontalis muscle, considering the patient’s age and sex, variants of aponeurosis location (classical, high, low), and the presence of hypertonicity (hypertonicity of the medial part, lower part, lateral fibers, total hypertonicity) [18]. Some possible combinations of points include: 3A, 3B, aB, aA; 3e, 3A, aB; 3A, 3B; 3A; 3B; 3A, aB; 3B, 3e; 3B, ae.
- When correcting wrinkles of the nasal bridge in special cases (eyebrow ptosis, facial nerve neuropathy with dystopia of the eyebrows and eyelids, eyebrow tattooing above their natural position), the BoNT-A injection point is the most sloped area of the glabella (forehead-nose junction). Injection points into the corrugator supercilii muscle should take into account anatomical structure variations: classical type, “feather-like”, and “high” type [16].
This scheme is applicable when using standard dilution protocols for BoNT-A preparations (according to the Instructions for medical use).
Additional information:
- Placing the thumb along the orbital rim may reduce the risk of diffusion of the product into the levator palpebrae superioris muscle during injection into the m. corrugator supercilii when correcting glabellar wrinkles.
- Skin stretching and lateral lighting help to identify vessels in the lateral canthus area.
Results:
The proposed marking of botulinum toxin type A injection points takes into account the anatomical and functional characteristics of the muscles involved in the formation of wrinkles in the glabellar region, forehead, and lateral canthus area, as well as the severity of facial wrinkles in men and women with high foreheads. For hygienic reasons, the applied markings must be removed before injections, which results in the loss of the advantage of topographic landmarks. Performing injections according to the proposed method allows experienced practitioners to avoid preliminary graphical marking of injection points due to the use of external anatomical landmarks – the eyebrows and eyes. Accumulation of experience in using this marking method will make it possible to evaluate its effectiveness in terms of preventing cosmetological complications during botulinum correction of the upper third of the face.
Conclusions:
- The proposed mapping scheme for the upper third of the face is simple, convenient, universal for beginner specialists, and is characterized by effectiveness and safety.
- The described method of injection point marking allows prediction of favorable outcomes of botulinum therapy for wrinkles of the upper third of the face.
References:
- Belyy I. Correction of facial expression wrinkles using Botox: the author’s “live face” technique. Cosmetics and Medicine. 2006; (5): 46–51.
- Borisevich I.V. Marketing analysis of the cosmetology services market in a large city. Dissertation for the degree of Candidate of Medical Sciences. Saint Petersburg; 2006. 157 p.
- Volkova O.V. Medical and social characteristics of adolescents with dermatocosmetological pathology and ways to optimize specialized care for this patient group. Abstract of dissertation for the degree of Candidate of Medical Sciences. Saint Petersburg; 2005. 22 p.
- Golubev V. The face from the perspective of its attractiveness (based on lecture materials for cosmetologists). KOSMETIK International. 2015; (2): 138–144.
- Zattler G. Aesthetic Correction of the Upper Third of the Face. Translated from German. Moscow: MEDpress-Inform; 2015. 120 p.
- Zolotareva V.G., Gara A.V. Features of botulinum therapy for aesthetic indications in patients over 45 years of age. Injection Methods in Cosmetology. 2011; (4): 54–60.
- Lapatina N.G., Saromytskaya A.N. “Toxin signs”: compensatory activation of non-target facial muscles after botulinum therapy. Injection Methods in Cosmetology. 2015; (2): 90–100.
- Le Louarn C. Functional facial analysis and botulinum toxin injections for aesthetic indications. Injection Methods in Cosmetology. 2013; (2): 32–41.
- Razumovskaya E.A. Mapping of the upper third of the face: possibilities for optimizing botulinum therapy outcomes. Injection Methods in Cosmetology. 2015; (2): 76–88.
- Rodionov A.N. Dermatocosmetology. Lesions of the facial skin and mucous membranes. Diagnosis, treatment, and prevention. Saint Petersburg: Nauka i Tekhnika; 2012. 912 p.
- Sergeev Yu.D., Bisyuk Yu.V. Improper provision of emergency medical care (expert and legal aspects). Scientific and practical guide. Moscow: Author’s Academy; KMK Scientific Publishing Association; 2008. 399 p.
- Sorokina V.K. Cosmetology: A manual for physicians. Saint Petersburg: Foliant Publishing House; 2014. 408 p.
- Chaykovskaya E., Orlova O. Aesthetic facial correction: consequences and possibilities we are unaware of. Injection Methods in Cosmetology. 2010; (3): 40–48.
- Shelekhov S. An integrated approach to facial expression management using botulinum toxin type A. Injection Methods in Cosmetology. 2010; (4): 2–9.
- Sherer M.A. Features of a combined approach to male facial correction: botulinum toxin type A and volumetric fillers. Injection Methods in Cosmetology. 2015; (1): 26–37.
- Yutskovskaya Ya., Dvoryaninova I., Birko O. Correction of the glabellar region using botulinum toxin type A (Dysport). Aesthetic Medicine. 2012; (3): 349–358.
- Yutskovskaya Ya., Dikaya A., Birko O. Botulinum therapy of the periorbital region considering anatomical features. Correction of paraorbital wrinkles in patients with the Slavic eye type. Aesthetic Medicine. 2011; (2): 189–197.
- Yutskovskaya Ya., Eremenko I., Seibel A., Birko O. Prediction of botulinum therapy outcomes (Dysport) in the upper third of the face. Aesthetic Medicine. 2011; (3): 363–368.
Author: Olga KRASILNIKOVA, MD – Dermatologist, Cosmetologist
Editor: Nataliya CHAYKA – Editor-in-Chief of ESTportal
Translation: Nataliya CHAYKA
First published: 2016
Updated in line with current guidelines and relevant research: 2026